Support at Home’s design flaws are now a governance problem, outgoing watchdog tells Senate
Published on 30 June 2026

The Inspector-General of Aged Care used her final appearance before the Senate Community Affairs References Committee to put a number on what poor program design is costing the system: a $50 pair of crutches that ends up costing $1,800 once occupational therapy assessment and a three-month wait are factored in.
“We’ve just paid 36 times the value of that support that that person could have had right then,” Natalie Siegel-Brown told the committee’s inquiry into Support at Home.
For providers and boards, the figure illustrates a structural risk that goes beyond individual case delays: a funding and assessment architecture that actively works against its own cost objectives, pushing people toward more expensive residential and hospital care – rather than away from it.
An assessment tool that excludes clinical judgement from the decision
Siegel-Brown’s most pointed criticism concerned the Integrated Assessment Tool, which determines what support a person receives. She told the committee that aged care has become an outlier in Australian health policy by excluding clinicians from the actual decision-making step.
“From Medicare, chronic disease management to allied health access, Australia routinely trusts clinicians to determine who needs support and what that support should look like,” she said. “Aged care is now the outlier. It’s a system where clinical judgement informs the data entry, but not the decision.”
Under questioning from Senator Ruston about whether re-running a flawed assessment through the same algorithm would simply reproduce the same result, Siegel-Brown conceded the point. “Why would the second production from the algorithm be any different to the first?” she said. “Unless you’re manipulating what you put in.”
The urgency classification sitting on top of that algorithm has produced a workload alarm that should concern any operator managing capacity planning: of roughly 100,000 assessments conducted since the program began, only 129 people have been classified as urgent. Siegel-Brown attributed this partly to a points system in which a person needs five out of six criteria to qualify, with one criterion – having waited over six months in a small town or remote area – automatically excluding the majority of applicants by geography alone.
Co-payment model shows an 88% jump in hardship applications
Siegel-Brown directed sharper criticism at the means-testing model than at any operational delay. She argued the design ties co-payments to care needs rather than financial capacity, producing outcomes she called fundamentally inequitable.
“Two people with exactly the same income are asked to pay very different amounts simply because one is frailer, sicker or further along the trajectory of decline,” she said.
Hardship applications rose 88% in the program’s first two months, which is data Siegel-Brown read as a structural signal rather than a transitional glitch. “What this points to is not a failure of principle, but a failure of design,” she said. “Early data suggests that hardship is not an edge case. It’s at serious risk of becoming a structural feature of Support at Home.”
She acknowledged the government’s decision to exempt personal care – showering, dressing, continence support – from co-payments, but noted the exemption doesn’t extend to cleaning, meals, transport or social support, all of which remain billable under the model.
Not a funding problem – an administrative one
Despite the scale of the criticism, Siegel-Brown was explicit that she sees the issue as fixable within existing budget settings, not a case for additional funding.
“I want this to work,” she said. “I think the budget is enough to make it work.”
Her recommendations to the committee:
- Reform of the means test to remove co-payments for the lowest-income recipients
- A human override mechanism for the assessment algorithm
- Mandated pricing transparency from providers, and
- An end to counting Stolen Generations redress payments as assessable assets under home care.
This last point is an inconsistency given the same payments were exempted from residential aged care means testing in the recent budget. “We are penalising people for accepting an apology,” she said.
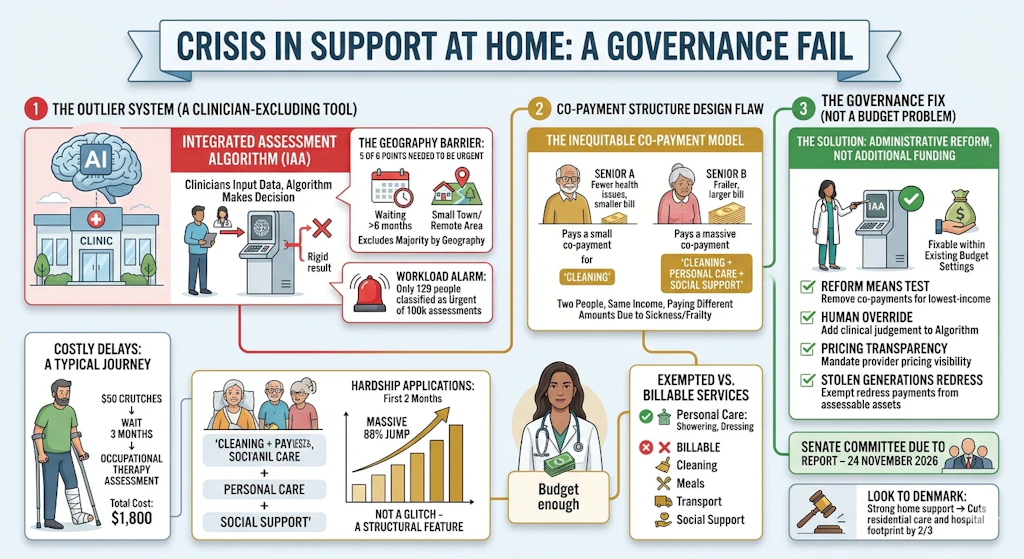
She pointed to Denmark as a comparative model: a home-support system effective enough that the country has legislated against building new residential aged care facilities and cut its hospital footprint to roughly a third of previous levels.
The Senate committee is due to report on 24 November 2026.